
Dental Swellings: Assessment & Management in ED
Author: Ruby Fussell
Introduction
Dental swellings are a common cause of facial infections presenting to the emergency department. While many can be managed conservatively with antibiotics and dental referral, some carry significant risks, especially due to their proximity to the airway.
Prompt identification of red flags is crucial to prevent complications such as Ludwig’s angina and airway compromise.
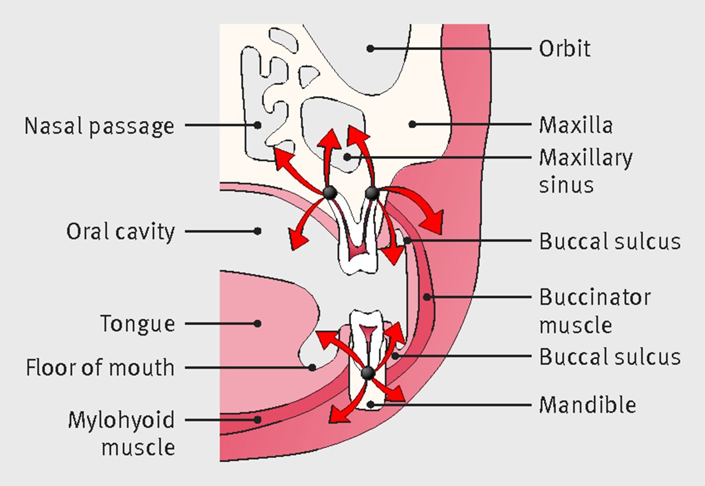
Figure one: spread of infection from dental sources is determined by fascial planes (Robertson DP et al., BMJ 2015;350:h1300, Fig. 3)
Causes of Dental Swellings
Dental infections typically arise from:
Tooth decay (caries) → pulp necrosis → periapical abscess
Periodontal disease → infection of supporting tissues
Pericoronitis → infection of the periodontal tissues surrounding partially erupted third molars
Failed dental treatment or trauma
Infection can spread into adjacent fascial spaces (see figure one)
Buccal space
Canine fossa (maxillary space)
Sublingual/submandibular/submental spaces
Severe infections may track into the parapharyngeal space, risking airway compromise
Clinical History
Key features suggesting a dental cause:
Localised toothache preceding swelling
Swelling in the jaw, cheek, submandibular, or submental areas
Recent dental work or missed appointments
Difficulty chewing or opening the mouth
Prior use of antibiotics or analgesia
Inflammation of the gingiva around partially erupted third molars
Important to establish the risk of severe infection:
Immunocompromised or diabetic status → increased risk
Examination
Use an A–E approach, with particular attention to signs of airway compromise.
Red Flag Features
Swelling crossing the midline (suggests submental involvement)
Raised floor of mouth
Trismus (mouth opening <10 mm)
Hoarse voice, drooling, or dysphagia
Tongue elevation or displacement
Difficulty speaking in full sentences
Local Examination
External: Look for erythema, tenderness, fluctuance, and cellulitis
Palpate: Can you feel the mandibular border? Any deep, fixed swelling?
Intraoral:
Tender tooth on percussion
Fullness in the gingival sulcus near the suspect tooth
Pus or discharge near molars
Raised mouth floor or asymmetrical pharynx
Ludwig’s Angina
Ludwig's angina is a serious and rapidly progressing bacterial infection, specifically a type of cellulitis, that affects the floor of the mouth and neck. The condition is characterised by bilateral, firm swelling of the submental and submandibular regions and the floor of the mouth, often accompanied by pain, dysphagia, trismus, and drooling. It can lead to airway obstruction and be life-threatening if not treated promptly.
Investigations
Bloods
FBC, U&Es, CRP
Glucose (especially if diabetic)
Blood cultures and venous blood gas if systemically unwell
Imaging
Orthopantomogram (OPG) – shows dental anatomy and apical pathology (see figure two)
CT neck with contrast – for deep space infection or airway concerns (see figure three)

Figure two: OPG demonstrating large apical lucencies to the roots of 37, the distal root of 36, and the proximal root of 38. Trace areas of surrounding sclerosis are also present. This patient presented with progressive left perimandibular facial swelling with tenderness to LL7.
Case courtesy of Sachi Hapugoda, Radiopaedia.org, rID: 57050

Figure three: CT neck demonstrates a fluid collection within the medullary cavity underlying teeth LL7 and LL8. There is an abscess in the left submandibular space extending into the parapharyngeal space, causing marked mass effect on the oropharynx.
Case courtesy of Steve Lau, Radiopaedia.org, rID: 28435
Immediate Management
For Well Patients with Localised Swelling
Oral antibiotics: Co-amoxiclav (or Clarithromycin + Metronidazole if allergic)
Advise to contact emergency dental services (via NHS 111 or GDP)
Safety-net: return if swelling worsening, signs of spreading infection, fever, trismus
If Red Flags or Severe Infection Present
Escalate to maxillofacial surgery urgently
Keep nil by mouth in case surgical drainage is needed
Start IV antibiotics: co-amoxiclav
Consider dexamethasone for airway protection
Analgesia and fluid resuscitation as required
Definitive Treatment
Incision and drainage under local anaesthetic for mild infections
Advise patients to seek definitive dental treatment from their general dental practitioner or via NHS 111 for the causative tooth
Admission for IV antibiotics and surgical drainage, and removal of the causative tooth under general anaesthetic in severe cases
Key Takeaways
Most dental swellings are benign and manageable with antibiotics + dental follow-up.
High-risk features require urgent referral:
Swelling crossing midline
Trismus
Raised mouth floor or protruding tongue
Hoarseness or drooling
Difficulty swallowing or speaking
References
Payne, K.F.B. et al. (2015) On-call in Oral and Maxillofacial Surgery, 2nd edn., Libri.
Edited from original article by Dr Ruby Fussell BDS MFDS (Ed)
Robertson DP, Keys W, Rautemaa-Richardson R, Burns R, Smith AJ. Management of severe acute dental infections. BMJ. 2015;350:h1300. doi:10.1136/bmj.h1300
Hapugoda S, Dental abscess. Case study, Radiopaedia.org (Accessed on 23 Jul 2025) https://doi.org/10.53347/rID-57050
Lau S, Mandibular abscess. Case study, Radiopaedia.org (Accessed on 23 Jul 2025) https://doi.org/10.53347/rID-28435