

JTG 2025 Poster Gallery
Revision Orbital Reconstruction - Outcomes with Patient Specific Implants
Introduction/Aims
The mainstay of treatment of symptomatic orbital fractures remains the reduction of herniated orbital contents and repair with a titanium plate. The management of patients who have had a stock plate with persistent symptoms is subject to debate. In this study, 15 patients underwent a novel analysis of orbital volumes (OV) and symptom assessment, prior to revision surgery with a patient specific implant (PSI).
Materials and Methods
Relevant cases were retrieved from clinical coding, operated between 2014 - 2020. After excluding 4 cases, 15 cases of revision reconstruction with PSI were analysed in detail, including pre-operative and post-primary-op signs and symptoms, and the outcomes after revision surgery with a custom implant. OV and Jaquiery class were calculated from CT images.
Results/Statistics
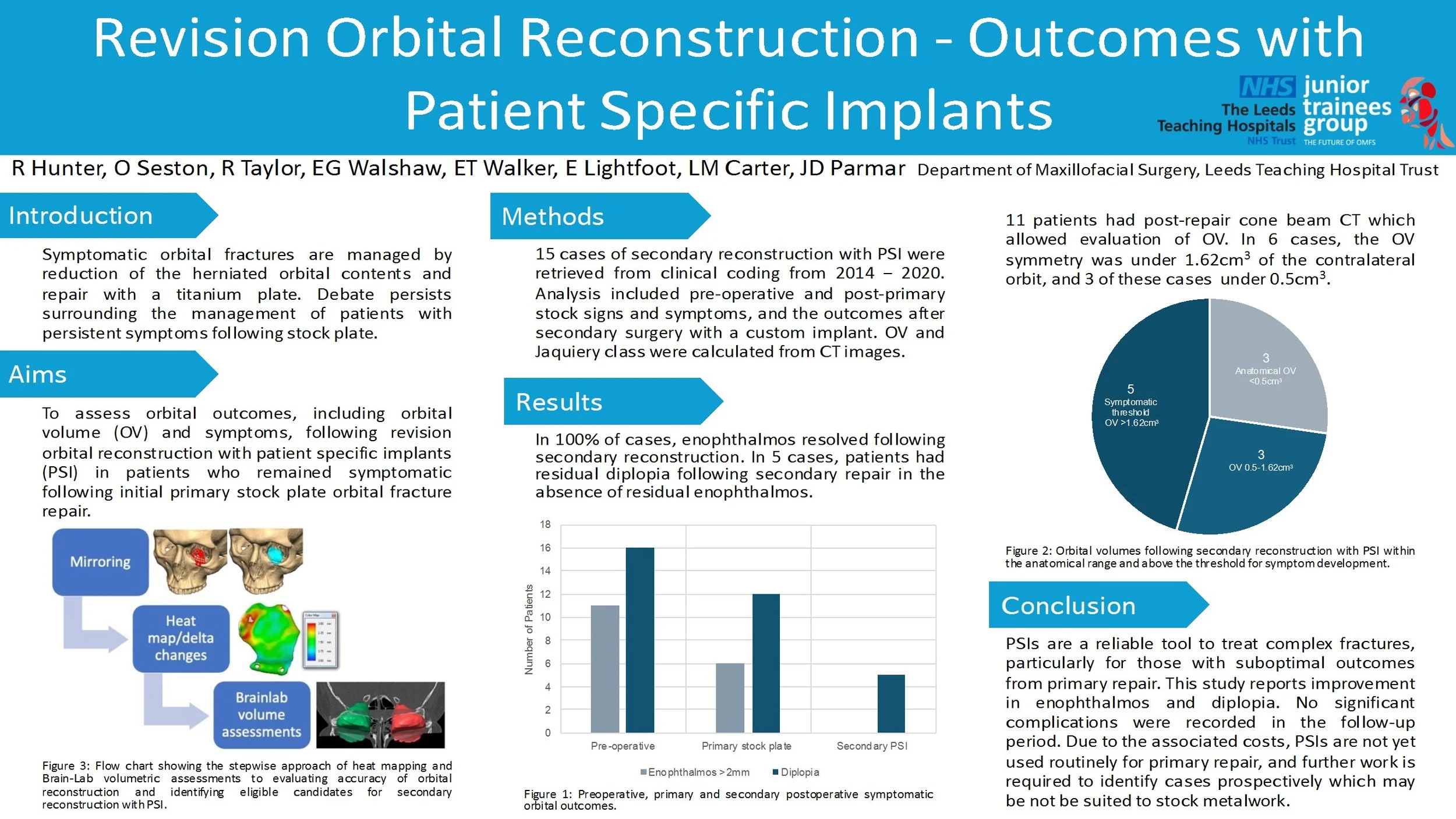
In 100% of cases, exophthalmos and hypoglobus resolved following revision reconstruction. In 5 cases, patients had residual diplopia following revision repair in the absence of residual exophthalmos or hypoglobus. 11 patients had post-repair cone beam CT which allowed evaluation of OV. In 6 cases, the OV symmetry was under 1.62cm3 of the contralateral orbit, and 3 of these cases under 0.5cm3.
Conclusions/Clinical Relevance
PSIs are a reliable tool to treat complex fractures, particularly for those with suboptimal outcomes from primary repair. This study reports good outcomes in terms of enophthalmos and hypoglobus with no significant complications in the followup period. Due to the associated costs, PSIs are not yet used routinely for primary repair, and further work is required to identify cases prospectively which may be not be suited to stock metalwork.

Reconstruction of Multifocal Comminuted Facial Fractures Caused by a Horse Kick
Introduction
Naso-orbital-ethmoidal (NOE) fractures are uncommon, complex facial fractures that
are often sustained following higher energy injury mechanisms. Common
mechanisms include road traffic accidents, sports injuries and horse kicks.
Anatomically, the NOE complex lies close to key facial structures including the orbits
and the anterior cranial fossa so damage to this complex can result in damage to
nearby structures. This can result in serious complications such as changes to vision
and intercranial infections.
Case Report
This case presents a 19-year-old patient who presented to the emergency
department following a horse kick to the face. Initial examinations revealed proptosis
and increased intercanthal distance. Imaging showed us that there were multifocal
comminuted fractures that involved the NOE complex, anterior cranial fossa, the
orbits, a retro-orbital haematoma, a small subdural haemorrhage and a small,
depressed skull fracture. The NOE fracture was determined to be a type 2 fracture
according to the Markowitz and Manson classification. Despite the severity of the
injuries, the patient remained GCS 15 throughout their care. For repair, an open
reduction and internal fixation using a coronal flap with cranialisation of the frontal
sinus was carried out.
Discussion
This case discusses the importance of early recognition and multidisciplinary
management of NOE fractures. Appropriate surgical intervention based on the
Markowitz and Manson classification is important in reducing complications such as
meningitis, facial deformities and ocular changes. Management of NOE fractures is
also important in order to achieve a good aesthetic outcome for the patient.
Training Bottlenecks in Oral and Maxillofacial Surgery: Insights from a UK Trainee Survey
Background
Recent findings from the British Medical Association reveal a national doctor unemployment crisis, with training bottlenecks exacerbating workforce underutilisation. In Oral and Maxillofacial Surgery (OMFS), extended training pathways and limited specialty training (ST) posts may heighten career uncertainty. Previous studies in BJOMS have highlighted training delays, gender disparities, and retention challenges, and the State of Play Report highlighted key issues including loss of agency, financial instability, and need to reform the current training pathway.
Methods
An online survey was distributed to OMFS trainees across the UK in July 2025. Questions explored current training stage, career intentions, application outcomes, job satisfaction, geographical mobility, perceived training bottlenecks, and wellbeing impacts.
Results
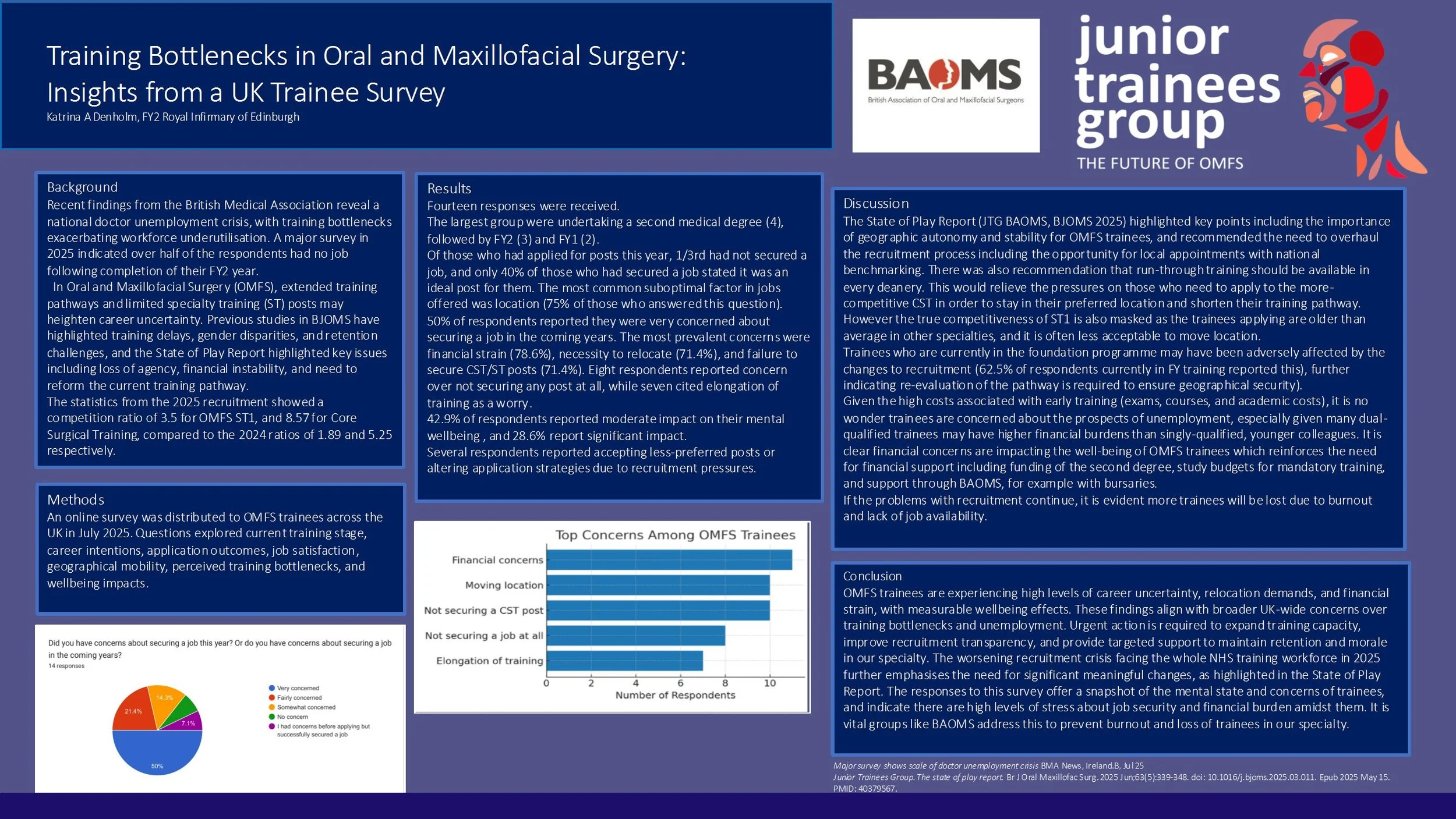
Fourteen responses were received. The largest group were undertaking a second medical degree, followed by FY2 and FY1. The most prevalent concerns were financial (78.6%), necessity to relocate (71.4%), and failure to secure CST posts (71.4%). Eight respondents feared not securing any post at all, while seven cited elongation of training as a worry. Wellbeing was moderately impacted in 42.9% and significantly impacted in 28.6%. Several respondents reported accepting less-preferred posts or altering application strategies due to recruitment pressures.
Conclusions
OMFS trainees are experiencing high levels of career uncertainty, relocation demands, and financial strain, with measurable wellbeing effects. These findings align with broader UK-wide concerns over training bottlenecks and underemployment. Urgent action is required to expand training capacity, improve recruitment transparency, and provide targeted support to maintain retention and morale in our speciality. The recruitment crisis facing the NHS workforce in 2025 further emphasises the need for significant meaningful changes highlighted by the State of Play Report.
Orthognathic Surgery Outcomes: A Regional Unit’s BAOMS Audit Findings
Introduction
The National Orthognathic Surgery Audit conducted by British Association of Oral and Maxillofacial Surgeons (BAOMS) aims to assess practice, quality of care, and outcomes throughout the UK. This retrospective audit presents findings from a regional maxillofacial unit, which contributed 35 patients to the national cohort of 947 from April 2024 to July 2025.
Methods
A review was conducted of all patients who underwent orthognathic surgery at our unit during this period. Data was collected on demographics, presenting complaints, diagnoses, treatment plans, surgical procedures, and postoperative outcomes.
Result
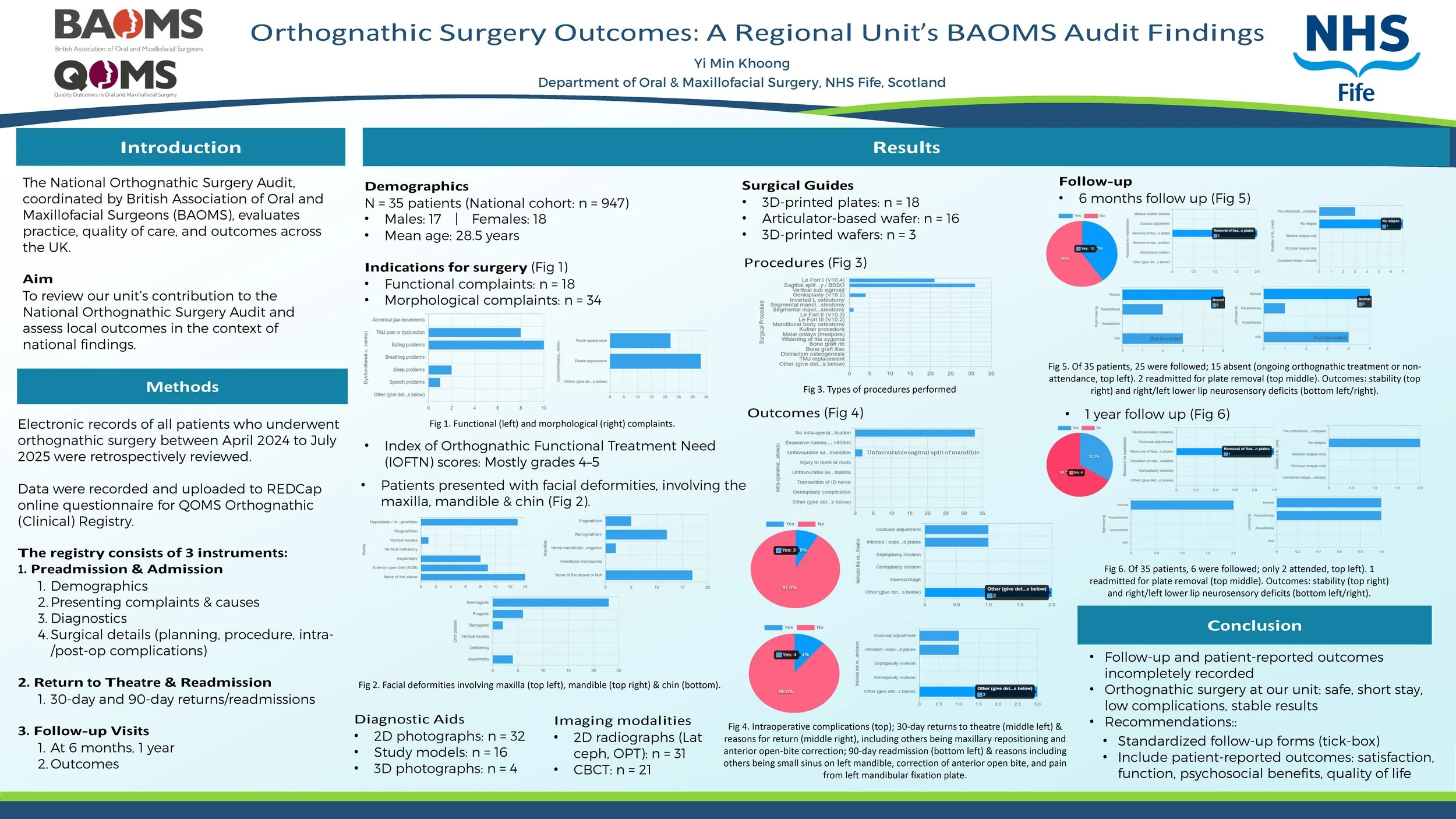
The cohort included 17 males and 18 females, with a mean age of 28.53 years. Indications encompassed functional issues (e.g., masticatory difficulties, TMJ dysfunction), and morphological deformities (facial, dental appearance). IOFTN scores were predominantly 4–5, reflecting high need.
The majority underwent combined procedures, most commonly Le Fort I osteotomy and bilateral sagittal split osteotomy, with a smaller proportion receiving genioplasty. Planning methods included both traditional and digital approaches, ranging from standard articulator-based techniques and wafers to advanced 3D planning with 3D-printed wafers.
The median inpatient stay was 1 day (range 0–2), with 10 patients discharged within 24 hours. Intraoperative complications were uncommon, with 2 cases of unfavourable sagittal split of mandible. A minority (5 patients) returned to theatre within 90 days, primarily for fixation plate-related problems and occlusal adjustments.
At follow-up, outcomes were stable with minimal relapse rates and acceptable neurosensory deficit. One readmission occurred within 1 year for plate removal. Documentation of follow-up and patient-reported outcomes was inconsistent across cases.
Conclusion
Orthognathic surgery at our unit demonstrates safe practice, short inpatient stay, low complication rates, and stable results. Follow-up documentation could be improved using a standardized tick-box, and patient-reported outcomes (e.g., satisfaction, functional and psychosocial benefits, quality of life) should be incorporated to better capture treatment impact.
In the Deep End: 2 Cases of Odontogenic Descending Necrotising Mediastinitis (DNM)
Introduction:
Descending necrotising mediastinitis (DNM) is a rare, potentially fatal, complication of a primary odontogenic or pharyngeal infection that spreads along the cervical fascial planes into the mediastinum. Odontogenic sources represent up to 58% of cases in some reports. This report describes the management of two patients with DNM.
Case Report:
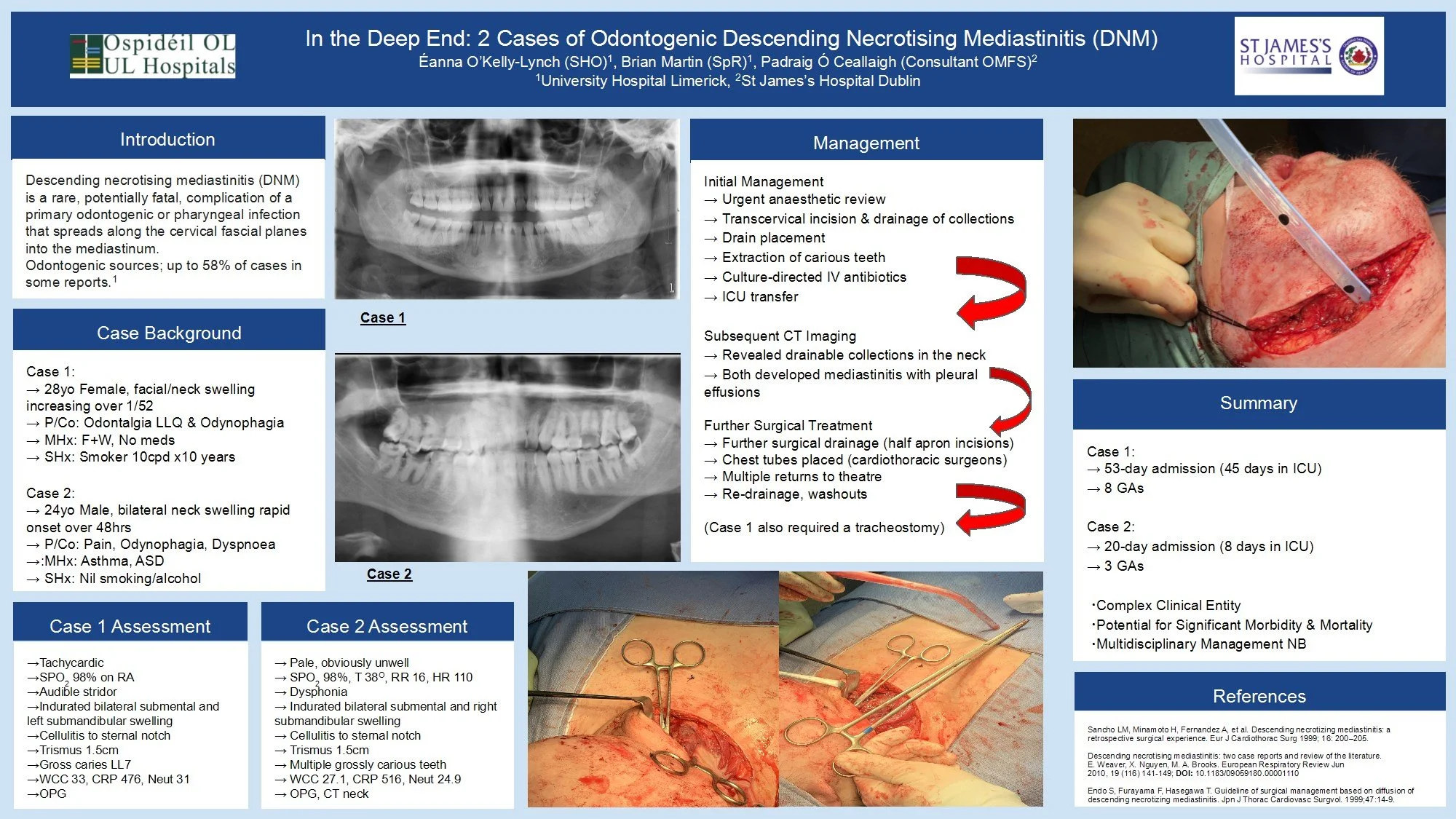
Case 1: A 28-year-old healthy female patient with one week of increasing facial and neck swelling, odontalgia and odynophagia.
Case 2: A 24-year-old male patient (asthmatic, ASD) with 48 hours of rapid-onset of bilateral neck swelling, pain, odynophagia and dyspnoea.
Both patients were tachycardic with indurated neck swellings and cellulitis, trismus, and grossly carious teeth. Bloodwork showed leukocytosis and elevated CRP.
Initial management for both involved urgent anaesthetic review, transcervical incision & drainage of collections with drain placement, and extraction of carious teeth. Culture-directed IV antibiotics were administered following ICU transfer.
Subsequent CT imaging confirmed the presence of drainable collections and need for surgical intervention. Both patients developed mediastinitis with pleural effusions, requiring drainage and placement of chest tubes.
Discussion:
Management of these cases required a multidisciplinary approach (OMFS, Cardiothoracics, Anaesthetics/Critical Care, Radiology, Microbiology) and both patients were discharged after extensive treatment courses.
Case 1: 53-day admission (45 in ICU), 8 general anaesthetics.
Case 2: 20-days admission (9 in ICU), 3 general anaesthetics.
Odontogenic infections, though common, have the potential for significant morbidity and mortality. DNM represents a challenging clinical entity that requires a prolonged and complex course of treatment. Oral and Maxillofacial Surgeons must be prepared to manage these cases and multidisciplinary input is essential.
Impact of Surgical Same Day Emergency Care (SDEC) on the Time to Surgery for Zygoma and Mandible Fractures
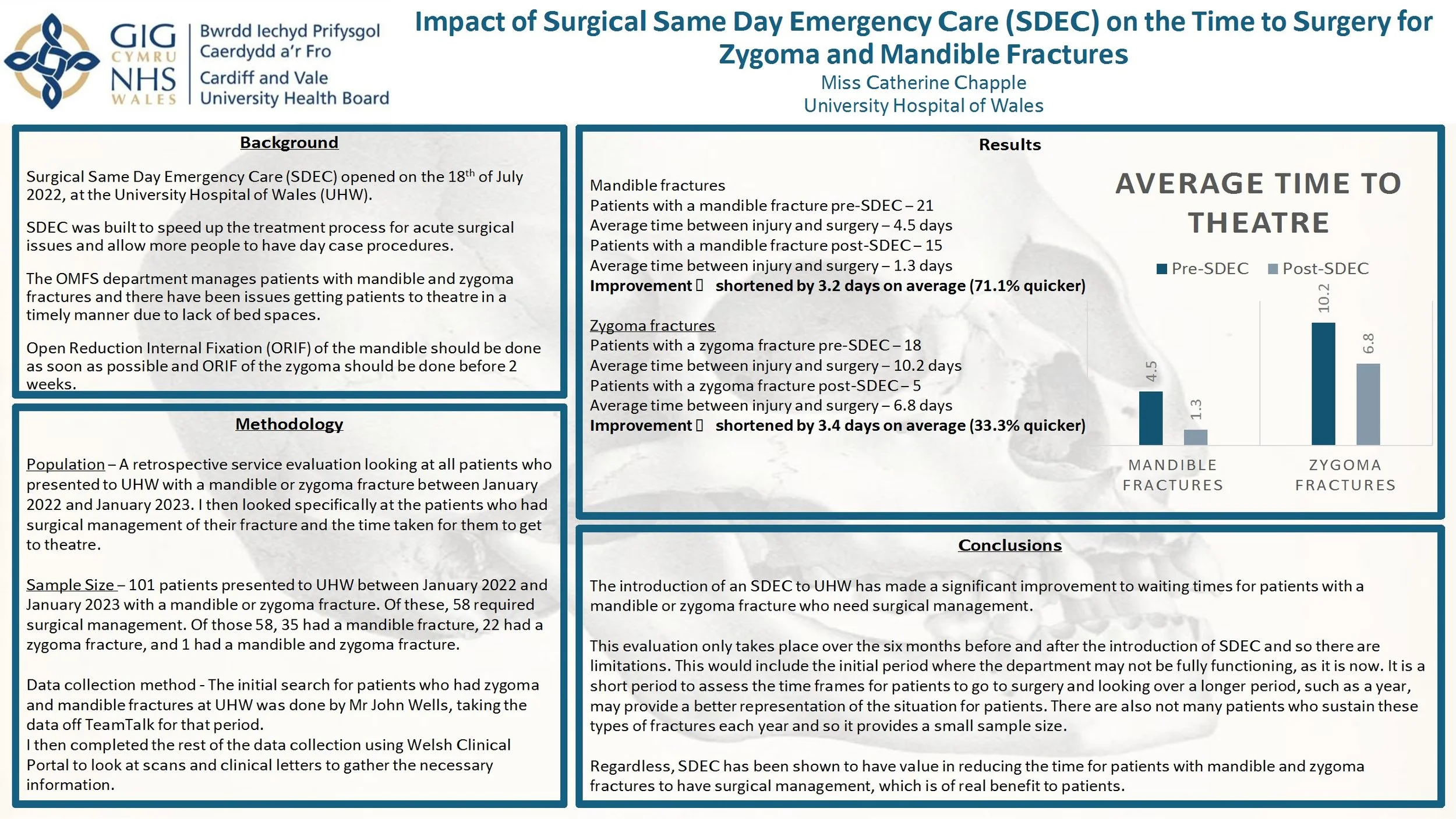
Introduction: Surgical Same Day Emergency Care (SDEC) opened on July 18th 2022 at the University Hospital of Wales (UHW). It aimed to accelerate the treatment process for acute surgical procedures and allow more day case procedures. The OMFS department manages patients with mandible and zygoma fractures and there were delays to surgical management due to lack of bed spaces. Open reduction internal fixation (ORIF) of the mandible should be done as soon as possible and ORIF of the zygoma should be done before 2 weeks. This service evaluation investigates whether the opening of SDEC had an impact on the waiting times for patients with mandible and zygoma fractures to have surgery.
Method: This is a retrospective service evaluation looking at all patients who presented to UHW with a mandible or zygoma fracture between January 2022 and 2023. I looked specifically at patients who had surgical management. The initial search for patients was done by taking data from TeamTalk and the rest of the data collection was from Welsh Clinical Portal.
Results: 101 patients presented to UHW between January 2022 and 2023 with a mandible or zygoma fracture. Of these, 58 required surgical management. Patients with a mandible fracture had their surgery 3.2 days earlier on average and patients with a zygoma fracture had their surgery 3.4 days earlier on average, after the implementation of SDEC.
Conclusion: The introduction of SDEC to UHW has made a significant improvement to waiting times for patients with mandible or zygoma fractures who need surgical management. However, this evaluation only looks at the management of patients 6 months before and after the implementation of SDEC and it is important to investigate over a longer period. Regardless, SDEC has been shown to have value in reducing the time taken to achieve surgical management.

An extensive Odontogenic Keratocyst in the left maxilla: a case report
Odontogenic Keratocysts (OKC) are benign cystic lesions that are known to be locally aggressive and have a high recurrence rate. Here we describe a case of a particularly extensive OKC.
A 28 year-old female presented to the Oral and Maxillofacial department with a 2-month history of facial swelling and pain. On examination, there was a left mid-facial swelling which was extremely tender on palpation, with intra-oral buccal expansion. Medically, she had depression and was a non-smoker. An OPG and CT neck with contrast was carried out; this revealed a substantial lesion, filling the left maxillary sinus, in association with a superiorly impacted UL8 tooth located just below the orbital apex. The lesion had cystic characteristics, measuring 6.6cm vertically, and 5.8 x 3.8cm in a transverse dimension. The lesion was shown to project medially into the nasal cavity, resulting in septal deviation to the right. Superiorly, there was associated convex bulging of the orbital floor.
Subsequently, antibiotics were prescribed; enucleation of the cyst and extraction of UL8 was carried out. The pathology result was in favour of Odontogenic Keratocyst. Infection reoccurred 1 month later which led to a washout of the cystic cavity, placement of a drain, extraction of a resorbed UL6 and additional antibiotic therapy. Gabapentin was then commenced due to associated neuropathic pain. 3 months following initial surgery, further enucleation of a 1x1cm residual cyst was carried out. 6 months later, a repeat CT scan revealed mildly progressive bony infill in line with ongoing healing and no evidence of recurrence.
This case highlights the aggressive nature of the OKC despite their slow growth. The presence of such an expansile lesion in the maxillary sinus with an associated ectopic tooth just below the orbital apex is rare. Close follow-up to detect recurrence is important.

Literature review: Intraosseous Hemangiomas of the facial bones: Diagnosis and management
Introduction
Intraosseous hemangiomas of the facial bones are rare benign tumours which are vascular in nature. This vascularity makes management difficult and often require a multidisciplinary approach for management. I have reviewed published literature to outline their presentation, the diagnostic tools available and management options.
Method
Articles were searched for by using pubmed medical database and reviewing articles references for similar articles.
Results
Intraosseous haemangiomas can present as painless bony lumps on the face or as space occupying lesions which compress structures, causing associated symptoms. These can include proptosis, facial deformity and dysethesia. Rarely they are painful. They can have differing vascular pressure, with a small number presenting as a pulsatile mass with bruit. There is no clear consensus on why they form, with a history of trauma and congenital reasons being suggested.
They are often first noted on CT imaging, showing heterogeneous honeycomb appearance. The benefit of MRI in diagnosis is disputed, as they can present as either high, low or mixed intensity on T1. However, MRI is useful to review vascularity within the lesion. Incisional biopsies have a limited role due to bleeding risk.
If no functional or aesthetic concern they can be managed conservatively. Non-surgical options attempted include needle aspiration, sclerotherapy and radiotherapy, all showing mixed results.
Surgical options are complicated by bleeding risks. This can be managed by removal ‘en-bloc’ to eliminate the need to enter the lesion, whilst pre-surgery embolization has also be utilised. Partial lesion removal has also been attempted, to restore function only.
Conclusion
Intraosseous hemangiomas of the facial bones are rare and limited published evidence exists, mainly case reports. There is not yet a consensus on the most useful diagnostic tools or their management. Each lesion presents its own challenges in removal and reconstruction dependent on size and location.
Too Many Calls? Auditing Emergency Department Referrals to OMFS
Introduction:
Emergency Departments (ED) frequently refer patients to Oral and Maxillofacial Surgery (OMFS). Many referrals are inappropriate or do not require specialist input. Unnecessary referrals increase workload, delay care, and strain resources. Local data on referral appropriateness are limited, making targeted interventions difficult. Evaluating referral quality is essential to ensure timely specialist care and optimise service efficiency. The aim of this study was to assess appropriateness of ED referrals to OMFS and ED staff confidence in the referral pathway.
Methods:
A retrospective audit was carried out over 21 days of ED referrals to OMFS. Referrals were categorised as appropriate, inappropriate, or uncertain using pre-defined criteria. Secondary outcomes included admission rates, cases managed with advice alone, and presentations suitable for ED or primary care. A short survey of 10 ED clinicians assessed confidence and familiarity with the OMFS referral pathway.
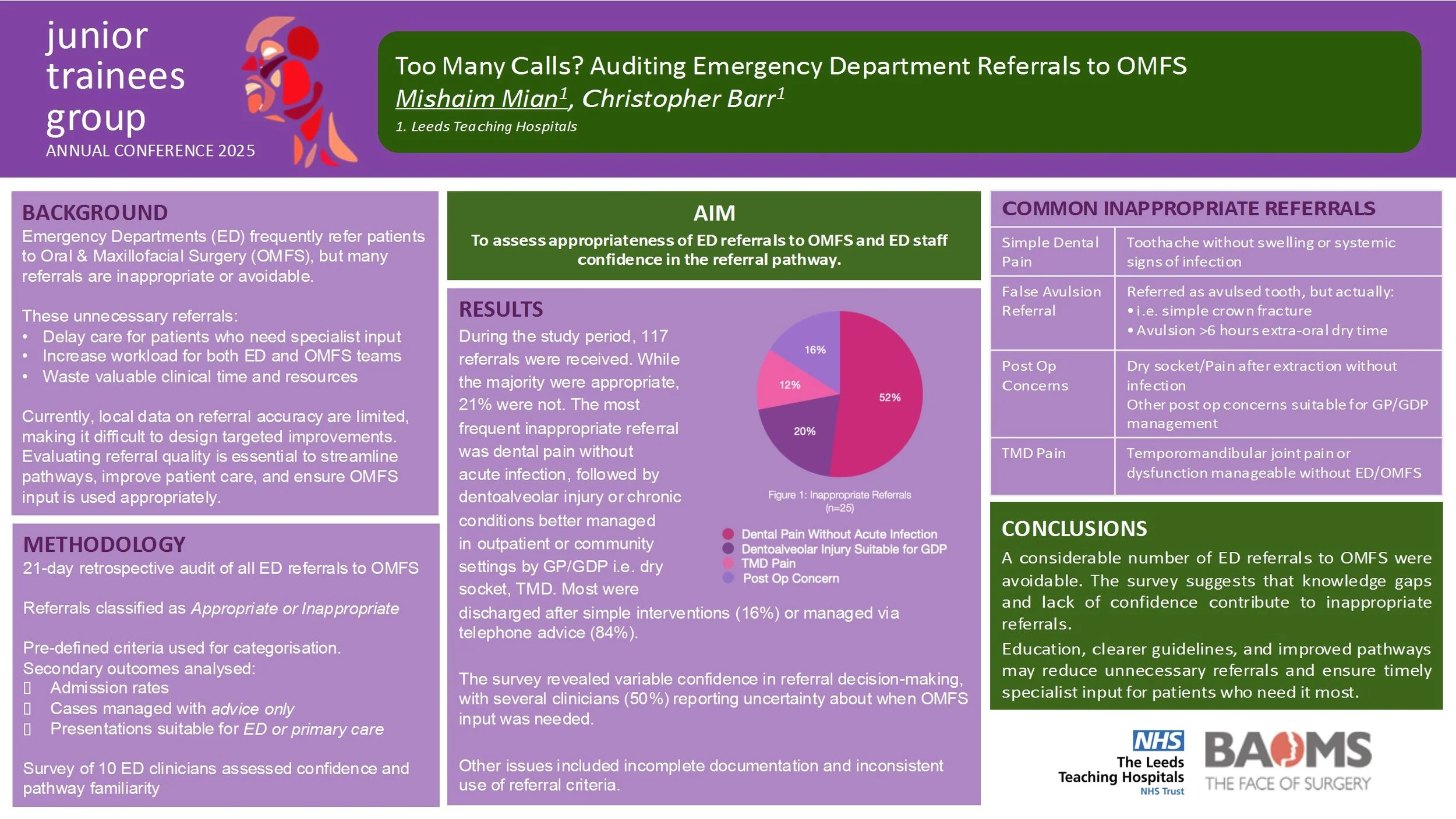
Results:
During the study period, 117 referrals were received. While the majority were appropriate, 21% were not. The most frequent inappropriate referral was dental pain without acute infection, followed by minor soft tissue injuries and chronic conditions better managed in outpatient or community settings. Only a small percentage required admission, while many were discharged after simple interventions or managed via telephone advice. The survey revealed variable confidence in referral decision-making, with several clinicians reporting uncertainty about when OMFS input was needed. Other issues included incomplete documentation and inconsistent use of referral criteria.
Conclusions:
A considerable number of ED referrals to OMFS were avoidable. The survey suggests that knowledge gaps and lack of confidence contribute to inappropriate referrals. Education, clearer guidelines, and improved pathways may reduce unnecessary referrals and ensure timely specialist input for patients who need it most.