
Maxillofacial Injuries
Maxillofacial Injuries
Face = ‘Crumple zone for Cranium’
Injuries + Complications:
Airway
Cervical spine
Bleeding
Head injury
Brain injury
Poly-trauma
Secondary Deformity
Commonest cause of carotid dissection in <25 year olds

Bungee jump → Rapid acceleration → Big pulsation in Carotid artery → Dissection
Implications of trauma
Litigation
Compensation to individuals who received surgery with substandard outcomes
Social implications
Newsworthy

Case of Princess Diana’s security, Trevor Rees-Jones having had facial reconstruction by French OMF surgeon Luc Chikhani following the car crash in 1997.
Key terminology
Laceration = wound caused by BLUNT TRAUMA
Different to a CUT
Edges irregular
Associated with bruising and often underlying hard tissue injury
Therefore when there’s a large cut, prior to stitching the skin, assess the area for a fracture
If fractures are missed there can be significant complications
Fracture of frontal bone in a patient could end up with a CSF leak and consequently a mucocele if not repaired beforehand
Stab = Depth > Width
Slash = Width > Depth
Hard Tissue fractures = Breakage of hard tissue (usually bone) either complete or incomplete
Simple = Clean break with minimal disruption to surrounding soft tissues
Compound = Fracture with breach of overlying soft tissues, usually skin but can be oral mucosa
Comminuted = Bone broken in ≥2 pieces, usually a reflection of the magnitude of the fracturing force (associated with a greater degree of injury (bone loss may need grafting/composite reconstruction)
Contaminated = Comminuted fracture with clear ingress of foreign body, much greater risk of infection = Poor prognosis
Classification of injury
Low impact - Blunt trauma - boot/fist/baton
High impact - Ballistic (high/low velocity) RTA pedestrian vs car often with poly trauma (neck/spine/limbs) - rare to see high velocity rounds, as will cause immediate mortality
Blast/explosion - Complex injury patterns, usually with burns, gross contamination
Gun powder in wound
Check for tissue loss, don’t chuck anything away ‘if black it can still be viable’
Drains to prevent dirty wound from becoming infected
Mixture of bony and soft tissue injury
Orbital Blowout fractures
Result of a direct blow to the orbit
Rapid increase in intraorbital pressure
Decompression occurs by fracture of ≥1 containing walls of the orbit
High index of suspicion and prompt identification important to prevent oculocardiac reflex in a trapdoor fracture (triad of bradycardia, syncope and nausea)
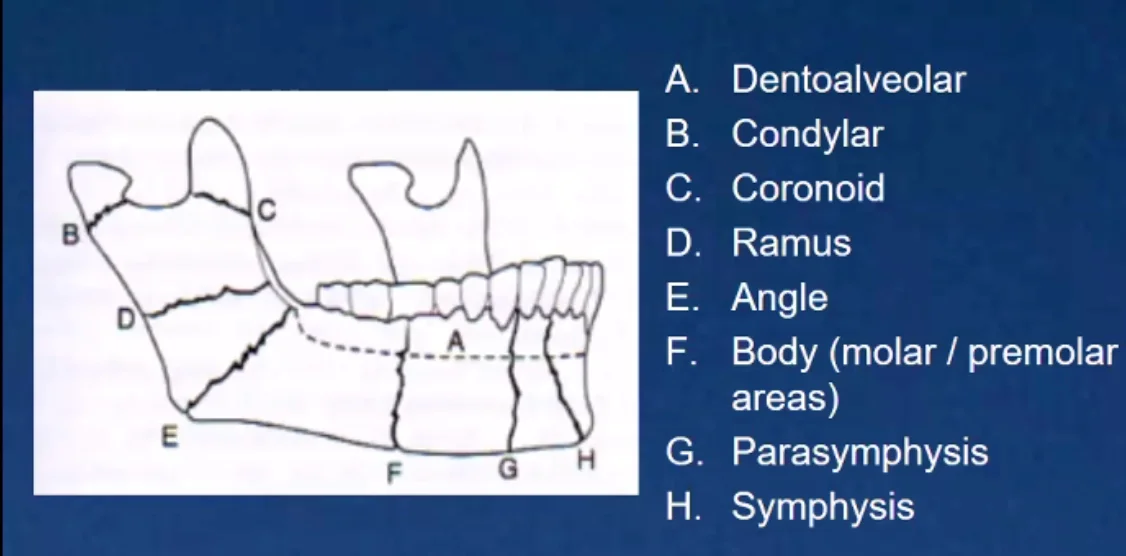
Mandibular fracture sites
Condyle is the commonest site of fracture
Fractures will typically occur at the weakest point of the bone
Angle and Symphysis also common
Le Fort Fractures (source radiopedia)
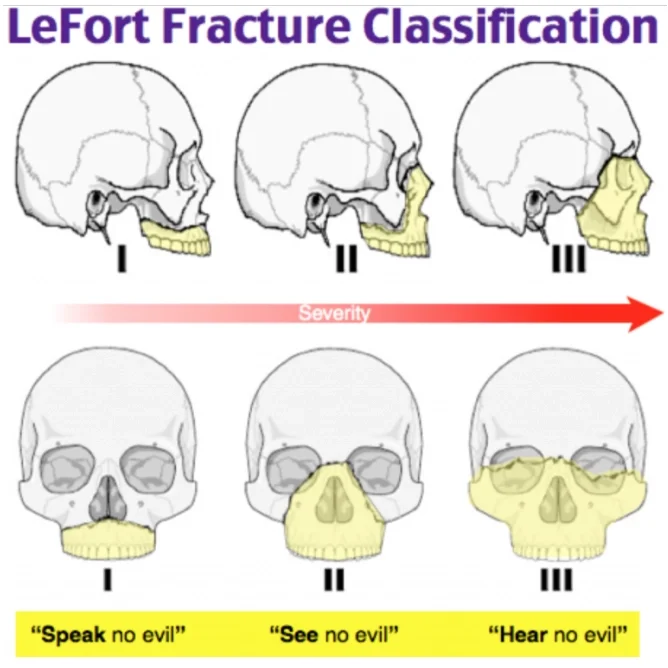
Discovered by Rene Le Fort applying blunt force of different magnitudes on cadaveric faces
Le Fort I 🙊
Horizontal alveolar ridge (tooth bearing part of maxilla)
Fracture line through alveolar ridge, lateral nose and inferior wall of maxillary sinus
Le Fort II 🙈
Pyramidal (nasofrontal suture apex + teeth are pyramid base)
Fracture arch passes through the posterior alveolar ridge, lateral walls of maxillary sinuses
Inferior orbital rim and nasal bones
Uppermost fracture line can pass through the nasofrontal junction or frontal process of maxilla
Le Fort III 🙉
Craniofacial disjunction
Transverse fracture line passing through nasofrontal suture, maxillo-frontal suture, orbital wall and zygomatic arch/zygomaticofrontal suture
Involvement of zygomatic arch, risk of temporalis muscle impingement
Type III fractures have highest rate of CSF leak
Memory aid:
Le Fort I is a floating palate (horizontal)
Le Fort II is a floating maxilla (pyramidal)
Le Fort III is a floating face (transverse)
Maxillofacial trauma examination
Start at the top and work your way down
Scalp → skull, forehead
Eyes → pupils, vision, position, movements
Ears → hearing, bleeding, CSF, haemotympanum
Zygomas → Deformity, steps, other signs of fracture
Nose → Deformity, bleeding, CSF, airway and septum
Maxilla → Solid or Mobile? Steps, bruising, swelling , bleeding
Mandible → Deformity, tenderness, bruising, swelling steps, movement, dental occlusion
Mouth to check for above + dental and dentoalveolar injuries
Soft tissue injuries → Site, size, nature, position, related structures
Facial sensation → Cranial nerve V (Va, Vb, Vc)
Facial movement → Cranial nerve VII (5 branches TZBMC)
Maxillofacial trauma aetiology
Interpersonal violence
Sports
Falls
RTA
Industrial accidents
Iatrogenic
Armed conflict/Civil unrest
Male:Female ratio = 2.1:1
Evidence based from BAOMS UK survery of facial injuries in 1997, BAOMS UK survey from previous decade echoes the same aetiology
Faris Ghafoor FY2